The Influence of Trust on Maternal Health Care in the U.S.
Individuals’ experiences during pregnancy, labor and delivery, and the postpartum period — both positive and negative — play a crucial role in shaping their trust in health care teams and the broader health system.2 In the patient-physician relationship, trust is defined as “an expectation that the other person will behave in a way that is beneficial, or at least not harmful, and allows for risks to be taken based on this expectation.”3 A lack of trust in maternal health care systems contributes to racial/ethnic inequities in perinatal outcomes (e.g., higher mortality rates and prolonged hospitalizations, among other outcomes).4 In order to make health systems work well at all levels, from individual interactions to large-scale operations, trust is widely understood as a key factor.5 6
The disruption of high-quality maternal health services during the COVID-19 pandemic, combined with growing attention to public trust in health systems and government institutions — particularly around the provision of respectful maternity care — has shaped emerging ideas, policies, and programs.7 This growing focus on trust is underscored by recent data revealing shifting public perceptions. Polls conducted by the AAMC Center for Health Justice from 2021-2024 on trust in institutions found a steady decline in the levels of trust in institutions such as health care systems, social service agencies, and other public institutions.8 These findings can have direct implications for maternal health. Given that a decline in trust can result in lower satisfaction for both patients and providers, and higher rates of disenrollment from care,9 gaining a deeper understanding of trust in maternal health care is essential. Maternity care that is patient-centered, prioritizes the individual’s needs, and demonstrates trustworthiness is more likely to enhance patient satisfaction and contribute to improved, more equitable health outcomes.10
This polling brief presents data from a nationally representative sample of adults, ages 18+ in the United States who have ever given birth (n=660)11 , examining levels of trust in health care providers during the perinatal period (pregnancy, labor and delivery, and postpartum) and adverse experiences encountered during labor and delivery. The poll was fielded in March 2025 and conducted using an online survey in English by Morning Consult.11 For the purpose of this brief, due to small sample sizes, racial and ethnic groups were categorized into two groups: (1) members of racial and ethnic minority groups (American Indian/Alaska Native, Asian, Black or African American, Hispanic or Latino, and Native Hawaiian or Pacific Islander adults) and (2) white adults.
Trust in Maternal Health Care
Respondents were asked whether they trusted their health care team to act in their best interest during the perinatal period. Overall, nearly all respondents reported trusting their health care team, with 97% reporting trust during pregnancy; 97%, during labor and delivery; and 96%, during the postpartum period. However, trust levels varied across demographic subgroups, particularly in pregnancy and postpartum care.
During pregnancy, respondents from younger generations — Gen Zers and millennials (96%) — reported lower levels of trust compared with Gen Xers and baby boomers (99%) (for more detail, see Supplemental Table 1). Trust in health care teams during the labor and delivery experience remained relatively stable across demographic groups, with no significant differences, but declined more noticeably during the postpartum period (see Figure 1). While the overall drop in trust from pregnancy to the postpartum period was 1.2 percentage points, the most notable declines were seen among Gen Zers and millennials (-3.7 points) and members of racial and ethnic minority groups (-3.3 points). These groups also reported lower overall trust during the postpartum period (92% and 93%, respectively), compared with members of the Gen X and baby boomer generations, and white respondents. These findings highlight a gradual decline of trust in health care teams as individuals transition from pregnancy to the postpartum period, emphasizing the need for focused efforts to sustain patient trust throughout the entire perinatal journey.
For a more detailed breakdown of trust levels by demographic subgroups, see Supplemental Table 1.
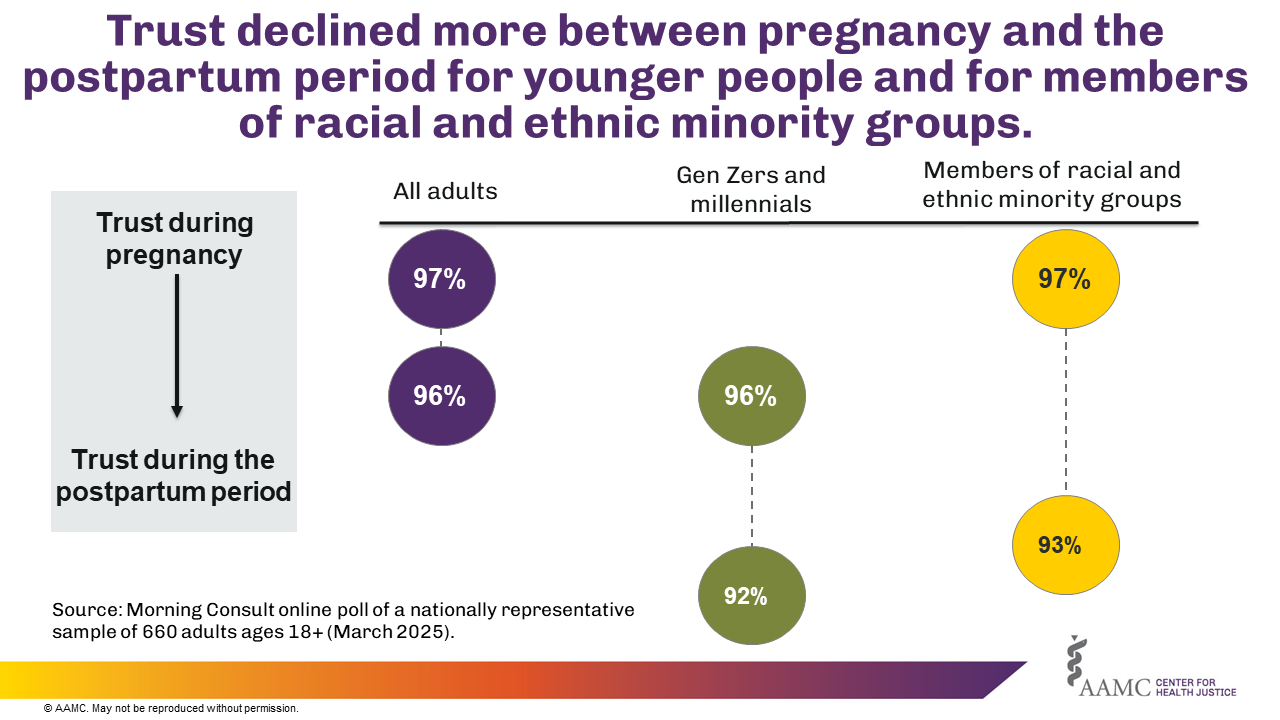
Figure 1
Negative Experiences During Labor and Delivery
Respondents were asked if they experienced any of the following during labor and delivery: mistreatment, disrespect, medical harm, being ignored, being dismissed, or coercion. Overall, 84% of respondents did not report experiencing any of the previously mentioned negative events. However, among the 16% who reported negative experiences, Gen Zers and millennials reported more frequent instances of medical harm (7%), disrespect (10%), being dismissed (12%), and being ignored (13%) compared with older respondents (Gen Xers and baby boomers). Similarly, members of racial and ethnic minority groups reported higher rates of mistreatment (7%), coercion in medical decision-making (7%), medical harm (8%), being dismissed (11%), and being ignored (11%) compared with white adults (see Figure 2 and Supplemental Table 2). While initial trust in maternal health care providers is high across all subpopulations, these findings suggest that younger adults and members of racial and ethnic minority groups reported negative experiences that can potentially accelerate declines in trust over time.
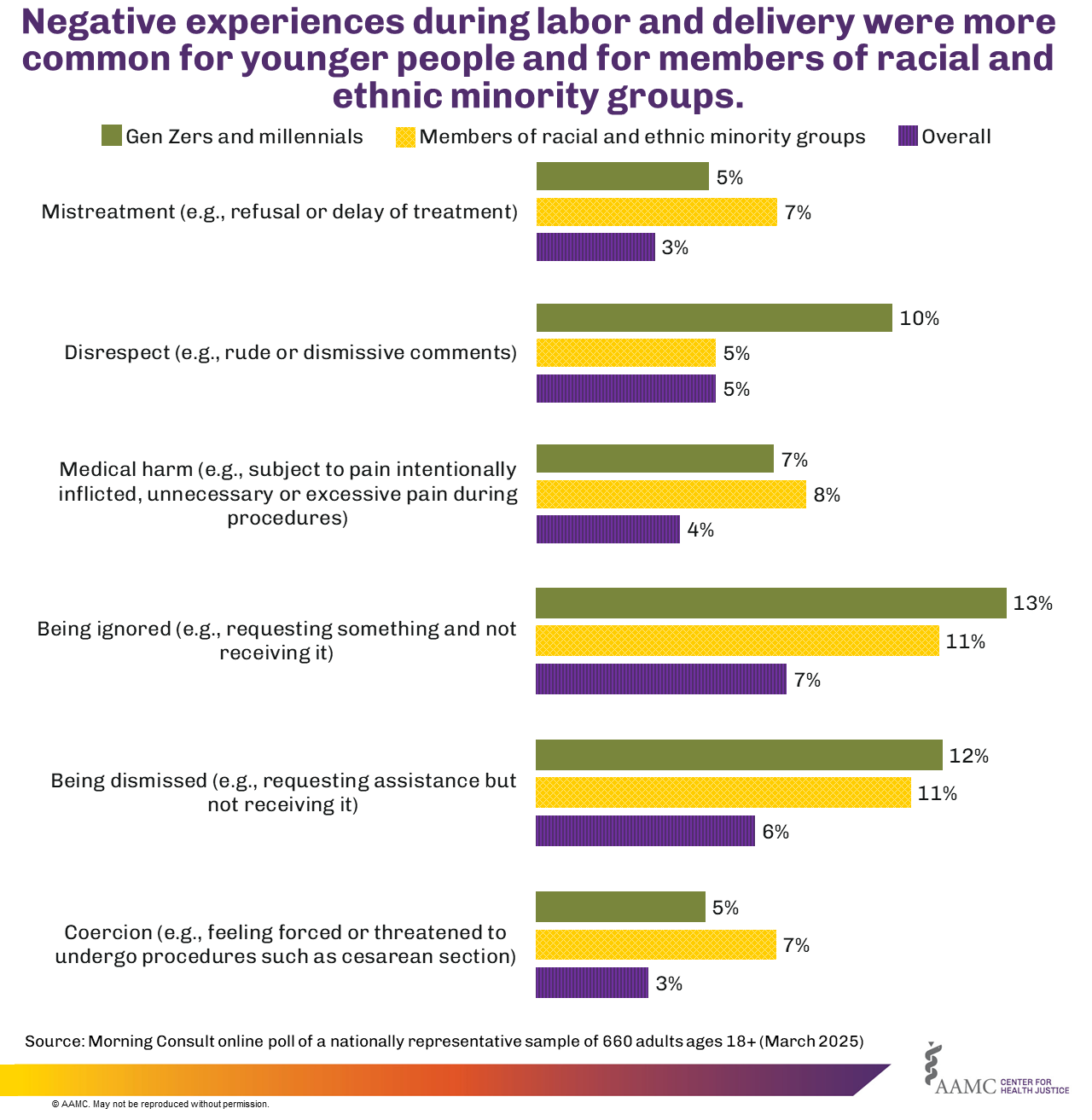
Figure 2
Actions to Improve Trust in Maternal Health Care
When asked to identify the most important actions health care providers could take to demonstrate trustworthiness, 97% of adults reported that providers should communicate clearly and honestly, demonstrate empathy, and respect patients’ choices and autonomy. Although members of racial and ethnic minority groups aligned closely with these priorities, they also emphasized two additional actions: actively listening to patients’ concerns and providing care tailored to the patient— both rated at 97%. Similarly, younger adults (Gen Zers and millennials) reported prioritizing respecting patients’ choices and autonomy (94%), demonstrating empathy (94%) and actively listening to patients’ concerns (93%) as their top priorities (See Table 1 and Supplemental Table 3). These findings underscore shared priorities across racial/ethnic and generational groups while also pointing to nuances in actions that different subpopulations find important when interacting with their health care providers.
Table 1. Top three important actions recommended for providers by all adults, younger adults, and members of racial and ethnic minority groups
| Ranked importance | All Adults | Younger adults | Members of racial and ethnic minority groups |
|---|---|---|---|
| 1 | Communicate clearly and honestly | Respect patients’ choices and autonomy | Communicate clearly and honestly |
| 2 | Demonstrate empathy | Demonstrate empathy | Provide care tailored to the patient |
| 3 | Respect patients’ choices and autonomy | Actively listen to patients’ concerns | Demonstrate empathy |
Strengthening Trust to Advance Equitable Maternal Health Care
Findings from this poll demonstrate that the vast majority of respondents reported very high levels of trust in their health care team throughout the perinatal period. This is especially noteworthy given persistent concerns about maternal health equity, such as the disproportionately high rates of maternal mortality among Black, Indigenous, Asian/Pacific Islander, and Hispanic individuals — which can erode trust in the health care system.12 13
Although most respondents reported high levels of trust in their health care team, trust was lower during the postpartum period compared with other stages of the perinatal experience (pregnancy and labor/delivery), with the most significant declines observed among younger adults and members of racial and ethnic minority groups. This pattern may be explained, in part, by negative experiences reported by the same groups during labor and delivery, including being ignored, dismissed, or medically harmed. Although a minority of respondents in our study reported negative experiences during labor and delivery, these negative experiences do occur.
For example, a recent study found that 1 in 6 people (17.3%) report experiencing one or more types of mistreatment during childbirth.14 This is similar to our 2022 From Pregnancy to Policy poll, which found that 20% of respondents rated their birthing experience as “Fair” or “Poor,” with Gen Zers more likely to report a “Fair” or “Poor” birthing experience. Although our current poll did not identify LGBTQ+ individuals, the 2022 Polling Spotlight: Understanding the Experiences of LGBTQ+ People Who Give Birth found that LGBTQ+ individuals also experienced “Fair” to “Very Poor” birthing experiences. While the findings from these polls are alarming, they also highlight critical intervention points for maintaining trust throughout the perinatal period.
Trust must be actively cultivated through patient-centered practices.15 Training providers to treat patients with kindness and respect can ensure that all individuals receive compassionate care and can strengthen trust in the health care system.16 Respondents identified clear and honest communication, empathy, and respect for patients' choices and autonomy as the top three most important provider actions to demonstrate trustworthiness. This emphasizes the need for health care teams to prioritize transparency, active listening, and respectful maternity care to sustain trust throughout the perinatal journey, particularly during vulnerable moments such as the postpartum period.17
More research is needed to explore how trust evolves throughout pregnancy, labor and delivery, and the postpartum period, and how it interacts with experiences of mistreatment and systemic inequities. To improve maternal health equity, efforts must also address system-level issues on maternal well-being, such as institutional trustworthiness and access to timely and respectful care. In addition, it’s important to note that, due to small sample sizes, we grouped racial and ethnic groups into a single category. We recognize this is a limitation, as each group has distinct histories, cultural contexts, and health care experiences. The findings in this brief indicate that these communities have different experiences, and future research should aim to disaggregate findings wherever possible.
Furthermore, efforts to address declining trust in maternal health care have been supported through interdisciplinary collaboration and innovation by the AAMC Center for Health Justice. In 2022, the Maternal Health Incubator focused on identifying missing data needed to advance maternal health equity. Responses emphasized the importance of patient and community voice, which led to the development of the 2023 Maternal Health Equity Workshop: From Story to Data to Action. The workshop centered on transforming lived experiences and qualitative information in medical records into actionable, data-informed strategies to help health professionals and advocates address disparities and rebuild trust. A key outcome was the creation of the Foundations of Responsible Natural Language Processing Use for Maternal Health Equity, guidelines for using natural language processing in ethical, inclusive, and community-responsive ways. These guidelines emphasize centering the patient’s voice, addressing bias in data sources, and ensuring that NLP tools support, rather than replace, human decision-making in maternal health care.
The Center is dedicated to supporting organizations and institutions in fostering trust and promoting health equity through collaborative efforts with community partners. By using tools and frameworks, such as the Center’s Principles of Trustworthiness Toolkit, health care providers and institutions can further enhance trust, paving the way for more equitable and patient-focused maternal health care. Other initiatives that promote trustworthiness, such as the Building Trust initiative from the ABIM Foundation,18 can support providers in fostering trustworthiness through empathy, transparency, shared decision-making, and meaningful patient engagement across the care continuum.
- Younger adults include individuals who were Gen Zers (born 1997-2012) and millennials (born 1981-1996). Members of racial and ethnic minority groups include individuals who identified as American Indian/Alaska Native, Asian, Black or African American, Hispanic or Latino, and Native Hawaiian or Pacific Islander. Back to text ↑
- MSD for Mothers. Integrating Women’s Experiences into Efforts to Improve the Quality of Maternity Care. https://www.msdformothers.com/docs/MSD-MfM-Brief-Integrating-Womens-Experiences.pdf. Accessed Mar. 20, 2025. Back to text ↑
- Thom DH, Wong ST, Guzman D, et al. Physician trust in the patient: development and validation of a new measure. Ann Fam Med. 2011 Mar-Apr;9(2):148-54. doi: 10.1370/afm.1224. PMID: 21403142; PMCID: PMC3056863. Back to text ↑
- Conteh N, Gagliardi J, McGahee S, Molina R, Clark CT, Clare CA. Medical mistrust in perinatal mental health. Harv Rev Psychiatry. 2022 Jul-Aug 01;30(4):238-247. doi: 10.1097/HRP.0000000000000345. PMID: 35849741. Back to text ↑
- Govender V, Topp SM, Tunçalp Ö. Rethinking trust in the context of mistreatment of women during childbirth: a neglected focus. BMJ Glob Health. 2022 May;7(5):e009490. doi: 10.1136/bmjgh-2022-009490. PMID: 35606016; PMCID: PMC9125697. Back to text ↑
- Rasiah S, Jaafar S, Yusof S, et al. A study of the nature and level of trust between patients and healthcare providers, its dimensions and determinants: a scoping review protocol. BMJ Open. 2020;10:e028061. doi: 10.1136/bmjopen-2018-028061. Back to text ↑
- Asefa A, Semaan A, Delvaux T, et al. The impact of COVID-19 on the provision of respectful maternity care: findings from a global survey of health workers. Women and Birth. 2021;35(4):378-386. doi:10.1016/j.wombi.2021.09.003. Back to text ↑
- Mendez, I, Alvarado CS, Alberti, PM. Trust Trends: U.S. Adults’ Gradually Declining Trust in Institutions, 2021-2024. AAMC Center for Health Justice. https://www.aamchealthjustice.org/news/polling/trust-trends. Accessed April 20, 2025. Back to text ↑
- Sheppard VB, Zambrana RE, O’Malley AS. Providing health care to low-income women: a matter of trust. Fam Pract. 2004;21(5):484-491. doi:10.1093/fampra/cmh5039. Back to text ↑
- Teisberg E, Wallace S, O’Hara S. Defining and implementing value-based health care: a strategic framework. Acad Med. 95(5):p 682-685, May 2020. doi: 10.1097/ACM.000000000000312211. Back to text ↑
- This poll of U.S. adults, ages 18+, was conducted by Morning Consult for the Center for Health Justice in 2025 (sample size: n=660) and was weighted to approximate a nationally representative sample based on individuals who have ever given birth. The poll was conducted using an online survey in English. Our analyses dichotomized having trust in the health care team into two categories: (1) “Agree” (“Strongly agree” and “Somewhat agree”) and (2) “Disagree” (“Strongly disagree” and “Somewhat disagree”). “I don’t know” and “No opinion” were removed. Similarly, we dichotomized the actions providers can take into two categories: (1) “Important” (“Very important” and “Somewhat important”) and (2) “Not important” (“Not too important” and “Not important at all”). “I don't know” and “No opinion” were removed. Back to text ↑
- Sen G, Reddy B, Iyer A. Beyond measurement: the drivers of disrespect and abuse in obstetric care. Reprod Health Matters, 26(53), 6–18. 2018. doi.org/10.1080/09688080.2018.1508173. Back to text ↑
- Howell EA. Reducing disparities in severe maternal morbidity and mortality. Clin Obstet Gynecol. 2018;61(2):387-399. doi:10.1097/grf.0000000000000349. Back to text ↑
- Vedam S, Stoll K, Taiwo TK, et al. The Giving Voice to Mothers study: inequity and mistreatment during pregnancy and childbirth in the United States. Reprod Health. 2019;16(1). doi:10.1186/s12978-019-0729-2. Back to text ↑
- Cometto G, Assegid S, Abiyu G, Kifle M, Tunçalp Ö, Syed S, Kleine Bingham M, Nyoni J, Ajuebor OK. Health workforce governance for compassionate and respectful care: a framework for research, policy and practice. BMJ Glob Health. 2022 Mar;7(3):e008007. doi: 10.1136/bmjgh-2021-008007. PMID: 35361661; PMCID: PMC8971763. Back to text ↑
- Urban Institute. Centering women’s voices to improve maternal health policies. https://www.urban.org/stories/centering-womens-voices-improve-maternal-health-policies. Published April 11, 2023. Accessed April 20, 2025. Back to text ↑
- Sudhinaraset M, Afulani P, Diamond-Smith N, Bhattacharyya S, Donnay F, Montagu D. Advancing a conceptual model to improve maternal health quality: the Person-Centered Care Framework for Reproductive Health Equity. Gates Open Res. 2017 Nov 6;1:1. doi: 10.12688/gatesopenres.12756.1. PMID: 29355215; PMCID: PMC5764229. Back to text ↑
- Building Trust Initiative. ABIM Foundation. https://buildingtrust.org/about/. Accessed April 20, 2025. Back to text ↑



