
From March 29 to April 3, 2022, the AAMC Center for Health Justice conducted a poll of a nationally representative sample of people in the United States who had given birth in the last 5 years. The poll asked questions regarding their pregnancy, birth, and postpartum experiences. The highlights of the poll were presented in a data brief published in May 2022, From Pregnancy to Policy: Birthing Experiences in the U.S.
About 13% of the sample identified with the LGBTQ+ community (including lesbian, gay, bisexual, transgender, queer, asexual, and other). In this polling spotlight, we highlight findings that significantly differed from responses of the cisgender, heterosexual population. We’re sharing this snapshot as part of our efforts to examine the perspectives of marginalized communities as we seek to build an inclusive health justice movement.
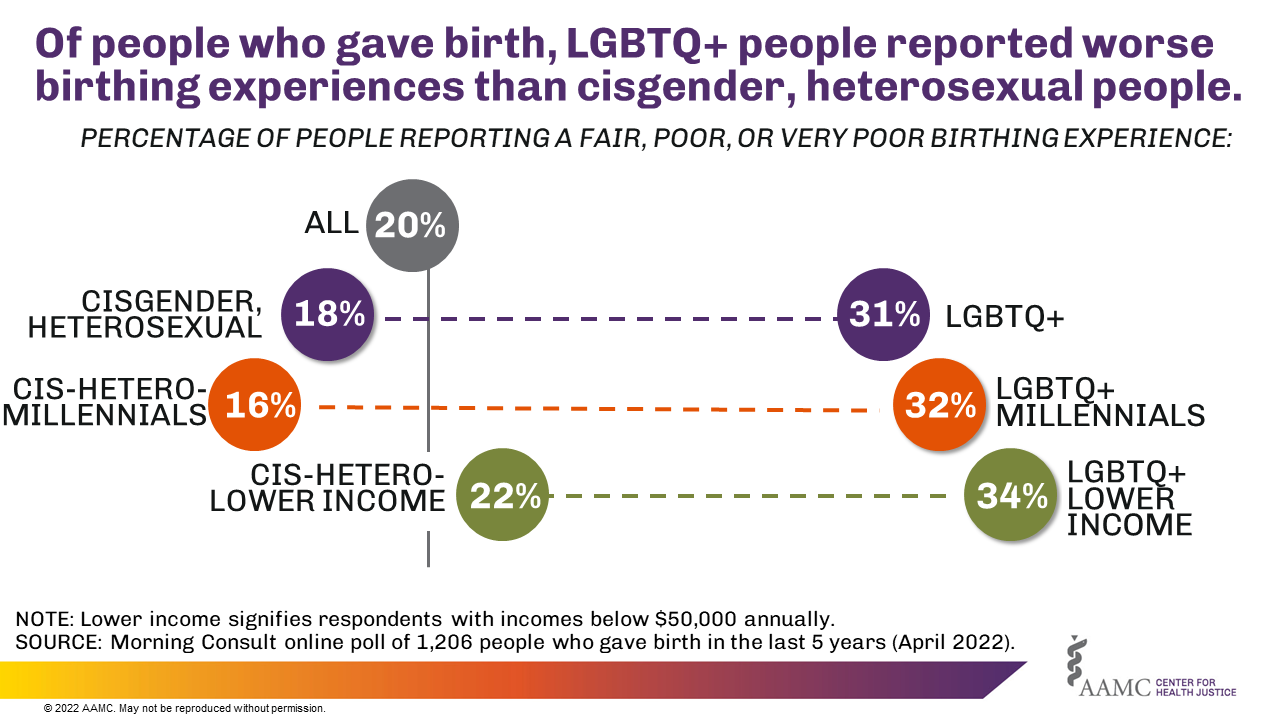
When asked to describe the overall childbirth experience, more LGBTQ+ individuals (31%) reported having a less than “good” experience (fair, poor, or very poor) than their cisgender, heterosexual counterparts (18%).*
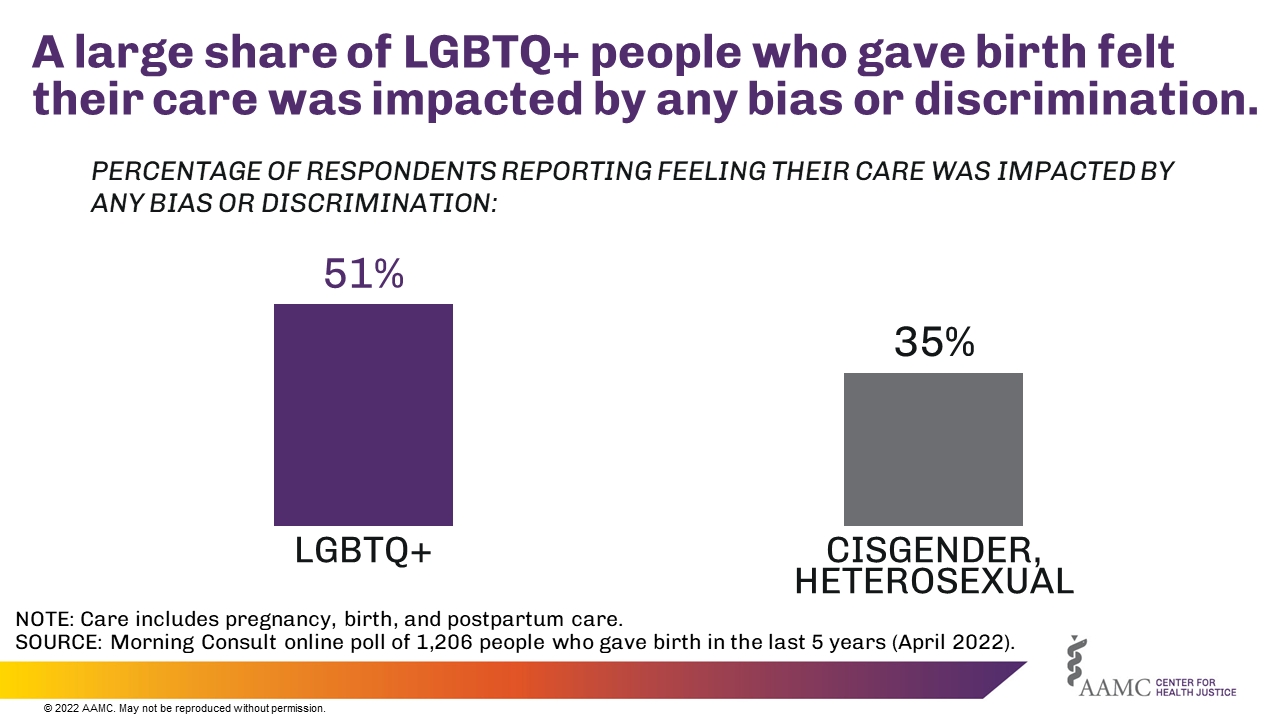
More than half (51%) of LGBTQ+ people who gave birth reported that the quality of their experience with pregnancy, birth, and postpartum care was impacted by bias or discrimination, compared to 35% of cisgender, heterosexual people, and 37% of all people who gave birth.
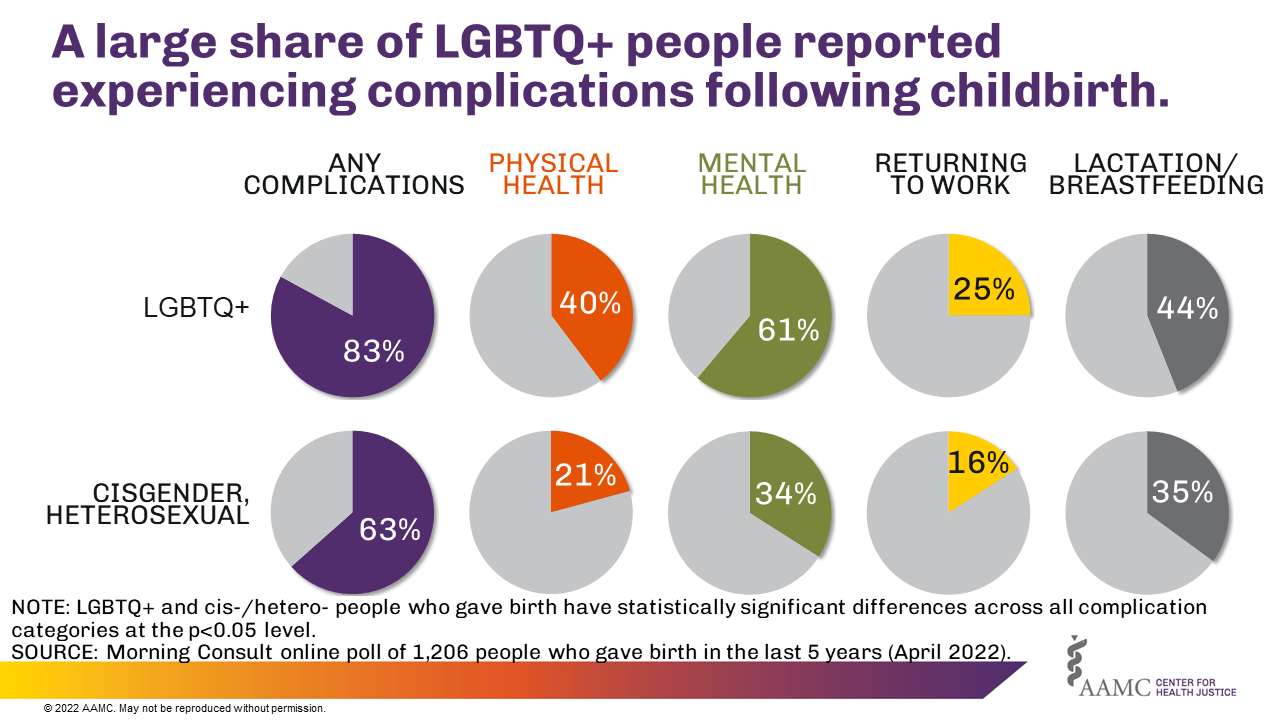
More LGBTQ+ people who gave birth reported complications with physical health, mental health, returning to work, and/or lactation/breastfeeding following childbirth compared with cisgender, heterosexual people.
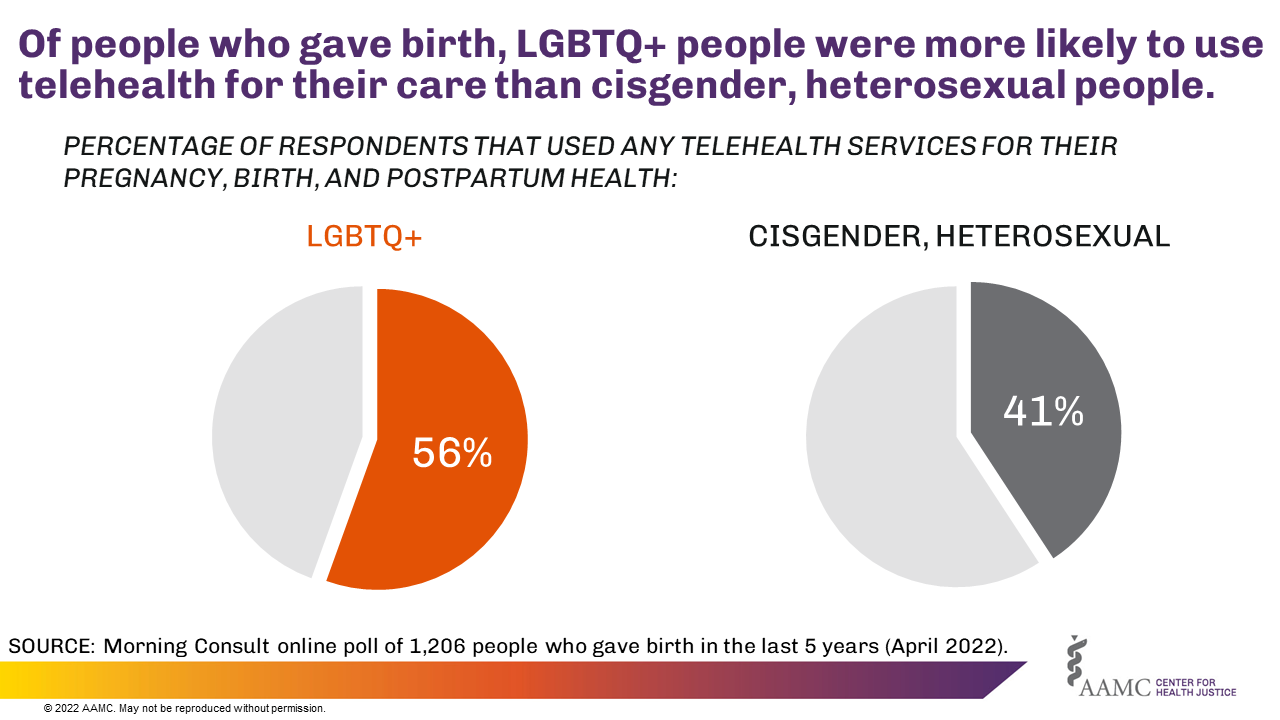
More LGBTQ+ people who gave birth (56%) reported using telemedicine/telehealth for services related to pregnancy, birth, and postpartum health compared to cisgender, heterosexual people (41%). Prior to the COVID-19 pandemic, LGBTQ+ people who gave birth were significantly more likely to use telehealth services compared to cisgender, heterosexual people who gave birth; however, during the pandemic, these difference were not significant.
Research has shown that the LGBTQ+ people experience perinatal care inequities ranging from limited access to care to adverse health outcomes.1,2
The LGBTQ+ community faces stressors like stigma and discrimination that impact their health and the health of their families. Adverse health outcomes including miscarriage, stillbirth, preterm births, and infants with low birth weight3 are higher for LGBTQ+ people who are pregnant or give birth. Physical and mental health are inextricably linked to one another, and LGBTQ+ people shoulder higher burdens of mental distress, anxiety, and depression.1,2
The drivers of these disparities range widely, from lack of access to culturally competent health care services to structural and interpersonal discrimination.4,5,6 Notably, the challenges individuals faced in the perinatal period are extensions of the negative and harmful experiences faced when accessing reproductive health care services.7 Moreover, the access to affirming mental health care for the LGBTQ+ community — especially during the perinatal period — is paramount for righting these inequities.
Solutions to these remediable issues must be system-wide, including the formal education and training of providers, and must incorporate organizations of all types demonstrating trustworthiness to the individuals in this community. Trustworthiness also means having knowledgeable, competent health care professionals delivering care, which happens by ensuring that the educational curricula as well as the research and evidence base8 upon which the curricula are developed are sound, responsive, and inclusive of the voices and perspectives of those from the community. Similarly, the social environments of health care organizations and institutions and their policies must be respectful and affirming, in order to serve the multiplicity of marginalized populations including the LGBTQ+ community.9,10 Due to the COVID-19 pandemic, telemedicine and telehealth have been thrust to the forefront of health care access and have proved to be a viable, reliable, acceptable, and welcomed mode of access, including for pregnant people, even those who are at higher risk of complications.11


