Experts have long believed that to achieve health equity across our communities requires a national, standardized data set that pulls together useful and actionable demographic, clinical, social, and other information to develop and evaluate multisector efforts. Government agencies are starting to invest in infrastructure for collecting and sharing health data to better understand and effectively intervene on community-level causes of poor health in communities that have been historically marginalized. These efforts will be more likely to succeed if they build on the public’s understanding and concerns around sharing personal, health-related information.
To help build the necessary foundation for this work, the AAMC Center for Health Justice polled a nationally representative sample of adults across the United States in January 2022 to learn about attitudes surrounding these issues. This data brief highlights key findings from the poll to provide actionable insights on trust and comfort levels around sharing personal information as well as the perceived impact of that sharing. All differences referenced are statistically significant.
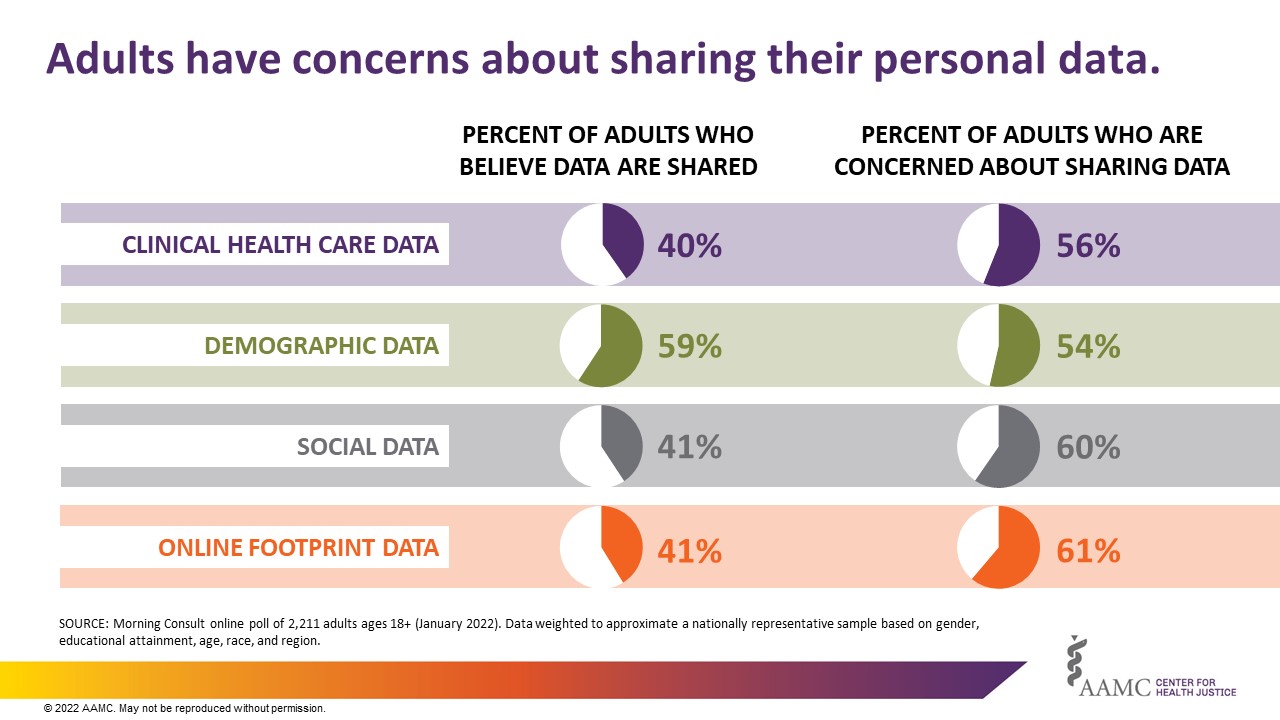
Many adults believe their personal information is being collected and shared, and concerns about this sharing are also consistently high across clinical, demographic, social, and online footprint data (Fig. 1). Most adults believe their demographic data is shared and are not concerned about it, but around 6 in 10 adults have concerns about sharing their social and online footprint data.
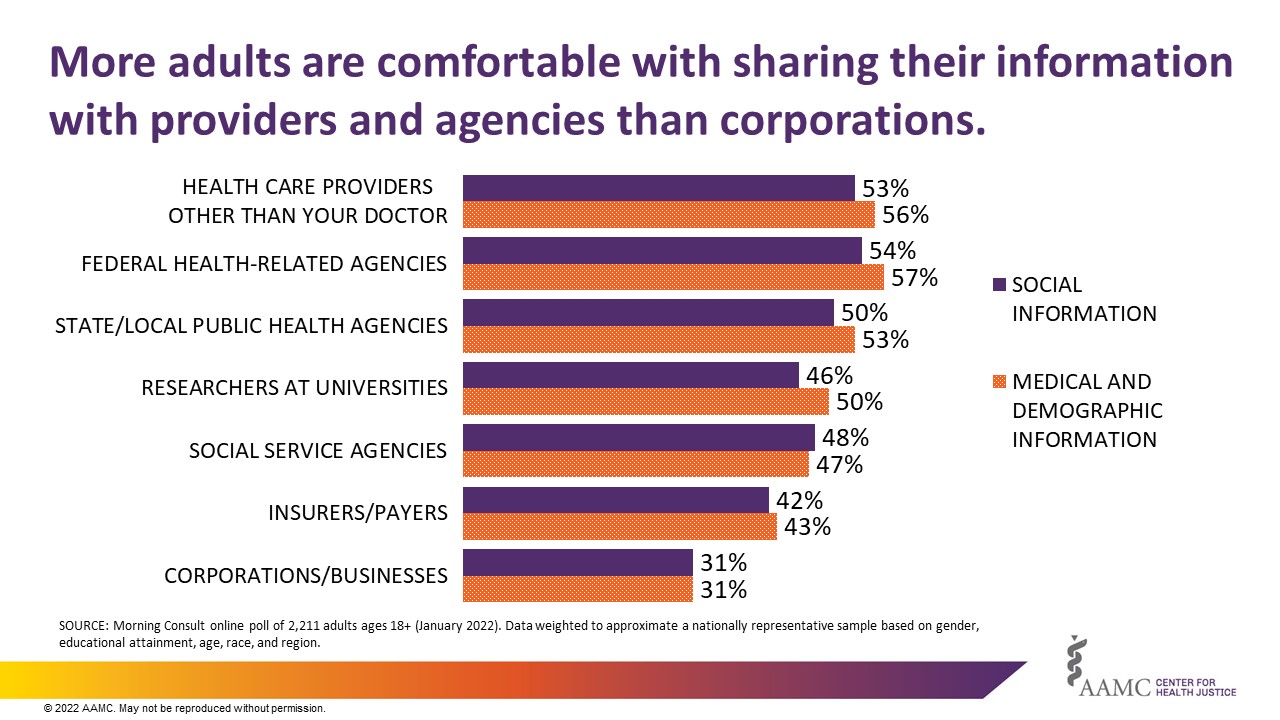
A person’s comfort level with their data being shared was also found to vary depending on the recipient of the data, with more adults willing to share with health care providers and state/local public health agencies as opposed to entities like insurers and corporations (Fig. 2). Regardless of the type of data, more than half of adults reported feeling comfortable sharing their information with health care providers other than their doctors, federal health-related agencies, and state and local public health agencies. However, less than a third of adults felt comfortable sharing their information with corporations or businesses.
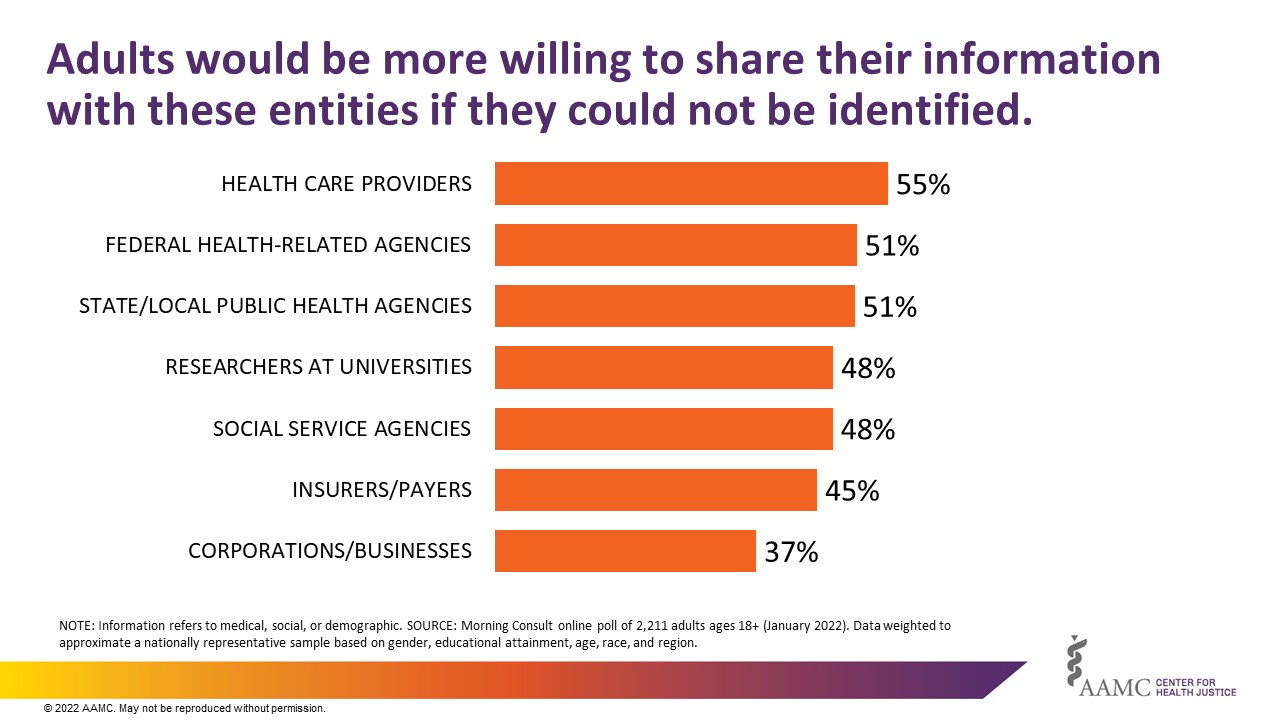
For a more thorough understanding of what might be leading to some of these attitudes around data sharing, adults were asked several questions about de-identified data that cannot be linked back to the individual from whom it was collected. Adults are more willing to share their information with all entities if identifiable information is removed: 37% would be more willing to share with corporations and 55% with health care providers. (Fig. 3). One in five adults don’t know if removing information that could easily identify them before it is shared would prevent recipients from figuring out who they are.
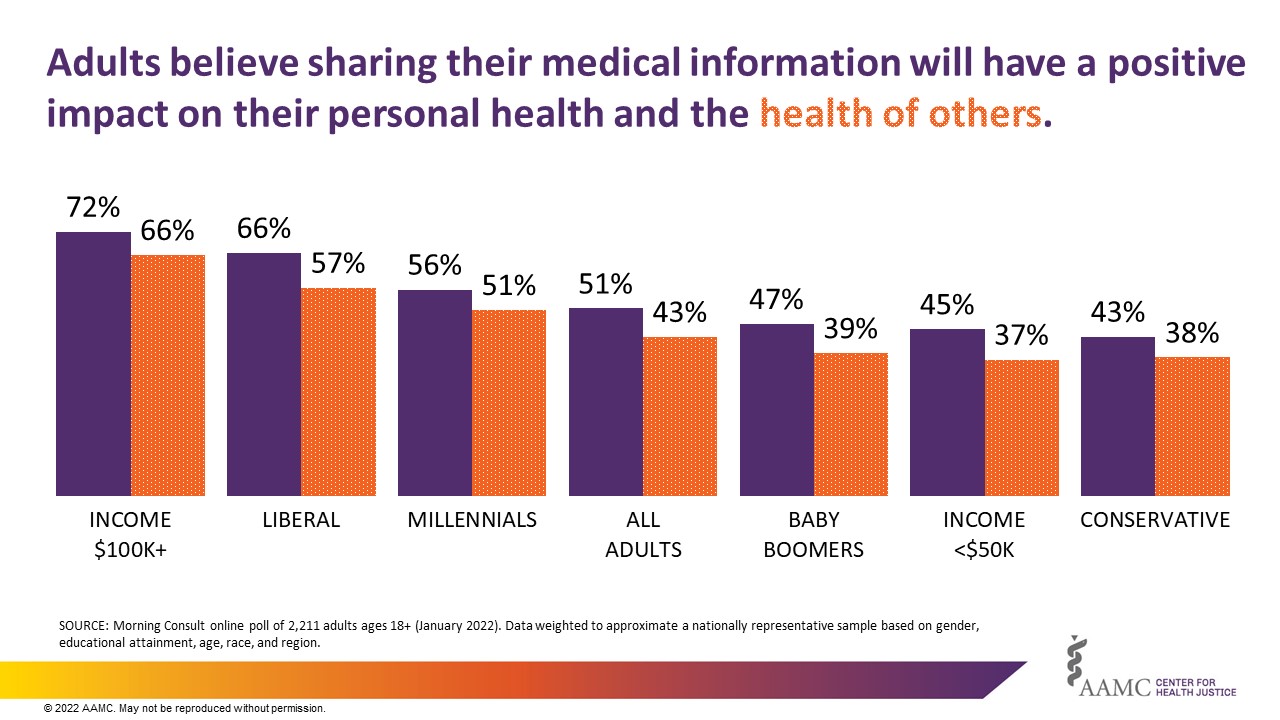
While many adults are mixed on the impact of sharing their information, certain demographics are more likely to think that sharing their information could have a positive impact on their personal health or the health of others — particularly those with higher incomes, those with liberal political views, and millennials (Fig. 4). This finding suggests that at a baseline, many adults are not aware of the opportunities that can come from sharing information about themselves. Engagement with communities around their concerns and the potential benefits of data sharing may be a key component in increasing acceptance within communities and diversifying the individuals represented in data sets.
Building the health justice movement for health equity means being as broad and inclusive as possible when we learn about communities. In part, that means working with communities to develop ways to best engage in local conversations about the benefits and risks of data collection, the most valuable and useful kind of data to collect, meaningful informed consent, and the ideal partners. Trustworthy data stewardship requires transparent communication around data collection that centers on the communities providing their information to ensure that data are inclusive of those who are vulnerable, in need of assistance, or impacted by inequities.
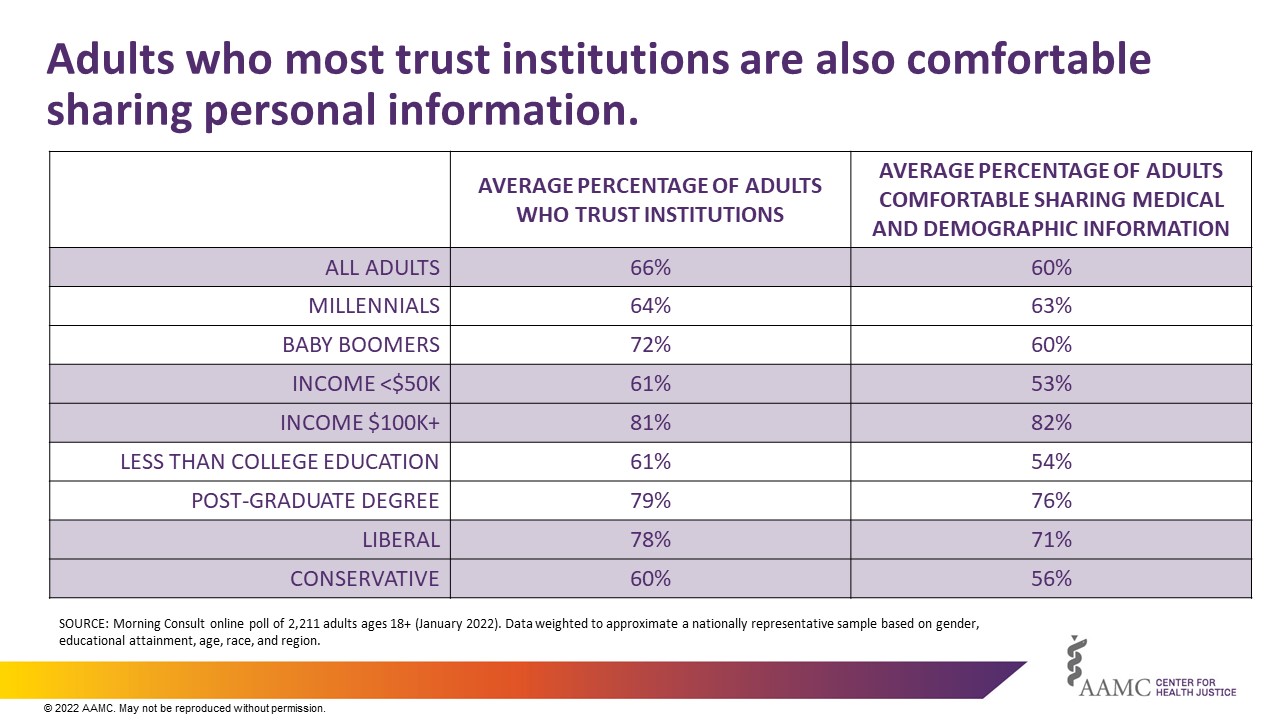
The trends identified in this poll about which institutions are most trusted by adults echo the findings from our last poll, The State of Trustworthiness. The overall data indicate that those who trust institutions within their community are also likely to be comfortable sharing their data (Fig. 5). These results highlight the importance of establishing organizations as trustworthy guardians of personal information in order to facilitate meaningful data collection and sharing, and they emphasize that we cannot lose sight of the perspectives of our communities as we shore up the evidence base for health equity.



